 There are many approaches to - or models of - counselling and psychotherapy, and many tribal wars about which is superior. This can be confusing for the public as they sift through the many offerings. The assumption throughout the history of counselling and psychotherapy is that it is the models, and the techniques based on them, which make theray effective. This assumption makes sense, given the emergence of therapy from medicine, wherein there is a disease with a cause, and technologies which assess and treat the disease. However, most of our personal struggles in life are not diseases, and this technocratic model is proving increasingly wrong for our needs. Meta-analytical research has now shown that most approaches to therapy are equally effective, but that what makes them effective is not the approach - the model and its techniques - but rather certain "common factors." This post is a summary of these factors. My goal in this essay is to report on the common factors theory, on how counselling in its effective essence is not the application of a medical or scientific model, but rather is a very honed way of doing something which is age-old. This will clear the ground for my next essay, in which I will argue that counselling is not inherently psychological, but rather that it is these common factors which do not rise to the specificity of any such discipline, which I will suggest can be blended with philosophical reflection to create philosophical counselling. The field of psychotherapy and counselling has traditionally focused on the models and techniques used by therapists, assuming that these are what make therapy effective. This focus is not true of all schools of therapy, for example existential therapy has a long tradition of criticising this assumption, however it has been the mainstream view. As above, this is due to the medical and technological culture in which therapy has emerged. However, overwhelming meta-analysis of the research has, in recent decades, revealed that models and techniques are not the key to change, and that they contribute a variance of only about 15%. It is other factors that make the difference, and these include client and extra-therapeutic factors (40%), the therapist and the therapeutic relationship (30%), and hope and placebo factors (15%). While models and techniques differ, these are the common factors that account for most of the good effect of therapy. This meta-analytic research is call "common factors theory." Common factors theory engages in a meta-analysis of the massive swathes of research now available to us regarding the outcomes of therapy and the factors involved. This gives us a picture of what is working not only in CBT or psychoanalysis or person-centred therapy, but in therapy as a whole. The pioneer of common factors theory was Michael Lambert. Below is his pie chart of which factors contribute to therapeutic outcome, and by what percentage. Later research, especially by Barry Duncan, enriched and complicated this model, however his equivalent diagram looks, in his own words, like a psychedelic artwork, so we will stick with Lambert's chart. Despite later developments by Duncan, especially in terms of a better recognition of what the therapist brings, nonetheless Lambert's diagram remains basically sound and is also easy to read. It should be noted that in this essay I use the words 'counselling,' 'therapy' and 'psychotherapy' interchangeably. 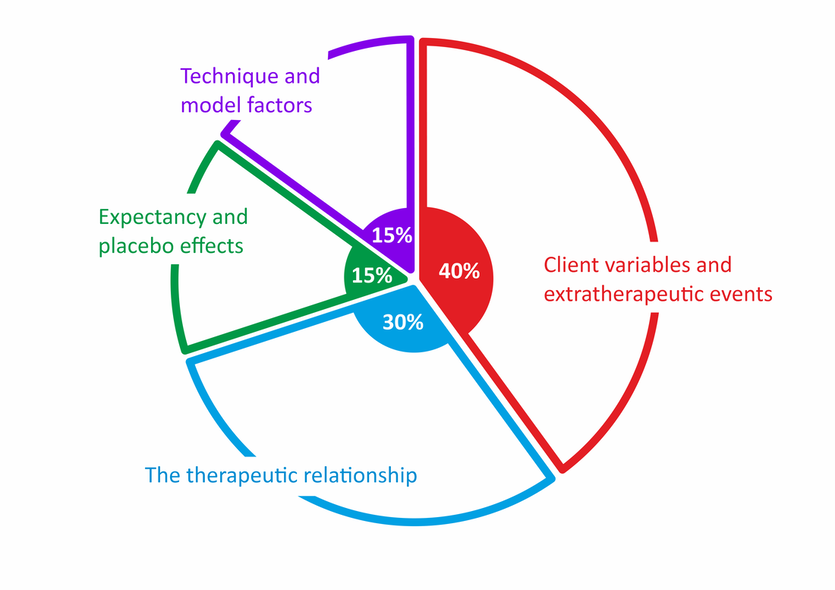 Client factors and extratherapeutic factors....
The biggest factor in therapy, according to the common factors research, is a mixture of what the client brings in terms of motivation and capacity, combined with the stuff that just happens to happen. Together these variables account for around 40% of the change in therapy, and they can be seen in red above. Let's start by discussing the extratherapeutic factors: the stuff that just happens to happen. I love the fact that happenstance plays such a big role in the change that is recorded through therapy. It challenges the hubris of us all - therapists and clients alike - that we have technologies which can give us control over life. The truth is that life and chance remain in control to some important degree. So many issues which clients have brought to me have been partly or largely resolved through unexpected or non-guaranteed events: an abusive partner suddenly ups and leaves; a lover suddenly appears in a lonely life; there is the offer a new job; or a life-changing delimma is resolved when an offer is withdrawn. All the angst that we were working on in therapy appears resolved. And in a sense it is. There is always deeper work to do, of course, in terms personal growth with regard to how you respond to problems and crises in general. In philosophical counselling there is also more work to be done because the therapy is about more than solving problems, it is about meaning and value and life purpose. However, it is certainly the case that "life is what happens while you are making other plans," to quote John Lennon, and that it is also what happens while you are working on things in therapy. The other common factor here is the client. This is where, in contrast to the above, we do something with what has been done to us. We face our challenges, and we make change happen within ourselves or out there. In more mundane terms, this factor refers to the quality of the client's participation, which the research (and common sense) shows is critical in determining the success of therapy. In this context the therapist's role is less about doing something to the client - certain assessments or diagnoses, or techniques or brilliant interventions - and more about helping the client to see themselves, to recognise and draw on their own strengths, resources, personal agency, and self-healing capacities. The therapist's role is merely facilitative, it is the client who contains the goods and who chooses to activate them or not, and who makes the effort to do so. I once worked hard for some time with a client on their many struggles with life, on their resentment and righteous anger, and on above their despair and sense of meaninglessness, and it slowly emerged that they were stuck and unhappy because at heart they said No to life as it is, at the existential level, at the level of the human condition. Although we could have done more work on this and I wish that we had, they left therapy soon after, having been confronted with their fundamental untenable stance toward life, and realising that they had no desire to change it in any way. Until they were willing to do so, they had no option but to be aggrieved and righteous. The things that a good therapist offers are powerful, but they have no power without the fundamental determination and courage of the client. As a therapist, I have long recognised that I am only as good as my client. Of course, the client might come to me feeling very confused, and they often do. But it is the client's efforts in using what I offer, which leads them to the benefits of what I offer. Passive people do not get much out of therapy, except perhaps to gain one more excuse, one more story to tell about being let down by therapists. Active clients can gain a lot from therapy. Of course, being active amounts to different things depending on the temperament of the client and what they want, and how that matches with the therapist. A person might walk away from the session without being able to define what happened, but simply feeling more free, clear and resolved. Another person gains some specific and important insight, which changes how they view and relate to an unchanging situation. Others change how they behave in the world, or make drastic changes in the structure of their life. All of these very different outcomes are expressions and results of active engagement. In therapy, it is really the client who does this for themselves. I am merely a resource. Therapist factors.... I mentioned that Barry Duncan extended the work of Michael Lambert. Duncan's very scientific graph looks like an acid trip, so I am using Lambert's pie chart, which fails to reference to this factor. Lambert, perhaps due to his radical paradigm shift away from the therapist as master to the client as hero, seems to have over-corrected and missed what the research shows about therapist factors. Therapist factors, in combination with the therapeutic relationship (below), provide 30% of the variance in therapeutic effectiveness. One might assume that the therapist factors refer to their therapeutic model and techniques, but those are different and we will come to them later. The research shows that it is more important who a client sees, than than what specific therapy is offered. "Some therapists consistently have outcomes superior to their peers. Evidence shows it is how they conduct therapy and not because of superior expertise in a model." Indeed, the research shows that age, gender, ethnicity/culture, profession/training, theoretical orientation, and experience are not common factors that contribute to therapuetic effectiveness. That's a radical outcome, and it throws a century of assumptions on their head. The factors that do contribute to outcome include: the therapist's facilitative skills (their ability to "draw forth" from a willing client), their interpersonal qualities, ability to connect, flexibility in meeting the client's way of being, and so forth. The research also clarifies that certain therapist behaviours undermine therapeutic outcome, for example confrontation, criticising the client, causing the client to feel attacked, blaming the client, projecting cultural arrogance and insensitivity, acting on negative emotions, assuming client perceptions versus inquiring about them, rigidity, and creating a poor therapeutic alliance. I find the common factors theory confirming of what I have always experienced and recognised as good therapy, versus therapy as mere technique which I have criticised for decades. There is, however, a surprise in the research even for people like myself, for it challenges our belief in the value of therapist experience, as per the sentence above. I believe confidently that decades of being a therapist has made me better at it. I often coach new therapists and I see the difference that experience makes. I also feel that part of what I offer to any individual client is a conversation which resonates with the insight of the thousands of deep therapeutic conversations I have had, especially when I have explored the same issue with hundreds or thousands of other people. I believe that many clients sense this in experienced therapists and value it. So how do we make sense of this suggestion that experience does not matter? Exploring this takes us a little deeper into some of what these common factors amount to. When I worked at Crisis Support Services, which ran telephone helplines (Suicideline, Mensline, Veteran's Line, and others) with paid, professional counsellors, I sometimes worked along 30 other counsellors on a shift, in an open-plan office where every counsellor could be heard if you sat close to them (the client could not be heard, the counsellor wore headphones). One learned a lot through over-hearing other counsellors. All these professionals had qualifications variously in counselling, social work, or psychology, with most being either qualified counsellors, or psychologists who were doing this job while completing the masters component of their studies. I met some great psychologists there. I also met just as many superficial and arrogant psychologists. The latter typically made it clear that they were superior to us mere counsellors, which is a common attitude. And yet, among all these different professionals on the phones, whom you could hear doing their work, the stand-out best were those with "mere" counselling degrees. Many of them had only diplomas, and were going nowhere beyond a low-paid job like this, and had no desire to go elsewhere as they valued this meaningful work. What was it that made them so much better than those masters and PhD-studying psychologists? Temperament. These people were counsellors "in their bones." They had a way of being with people that made all the difference. They had the right temperament. Training is needed to use this temperament in the right way, so that the conversation is actually a counselling one, with all the potential power of that, and so that both the counsellor's and the client's well-being is protected. Training is also useful insofar as, yes, ideas and techniques are useful, which they are with respect to a 15% variance. However, I would choose my own counsellor based on their temperament rather than the type or prestige of their training. Indeed, I value being in counselling as a lifelong enriching process, and so currently have my own ongoing counsellor. While I have a masters degree, he has only a diploma. It is his qualities as a person of substance, a man who is reflective, wise, and kind, which make him so good. A final word on this issue of experience. I suggest that what we call experience is often actually wisdom. Wisdom seems to me to be what comes of experience plus personal qualities. These personal qualities include curiosity and reflection, empathy, a concern for truth above personal ego, and so on. When we speak of experience, we are really speaking of wisdom, rather than mere quantitative experience. After all, there are plenty of old fools in this world, people who have merely existed while things have happened. Or who have responded to what has happened in foolish and egoistic ways, who have remained childish or become bitter. When we speak of an experienced therapist, really we are speaking of a wise therapist, somebody who internally does something with what they experience. The therapeutic relationship.... We just spoke of the therapist qualities, however the therapist is not an isolated object, rather the qualities we dicussed all point to their way of being with the client. The way of being together between the therapist and client is referred to as "the therapeutic relationship." The research shows that this relationship is also a fundamental factor in therapy, combining with therapist factors to contribute 30% of the effectiveness. Clients typically attribute the success of their therapy to their connection with their counsellors. As a lifelong client of counselling, having had mostly good experiences, a couple of average ones, and a downright abusive one, I have experienced the power of a good relationship with a therapist. The majority of these counsellors have taken up welcome real estate in my head, becoming a voice for reason, calm, wisdom, and meaning, boosting my direction and potential, and speaking up for my worth and boundaries. I know from feedback that I do the same for many of my clients. In a world where we internalise so many harmful voices, the counsellor becomes an internalised voice for good. Relationship matters. The world is a lonely place for many people. Plus, many have been harmed by relationships, whether with their parents, partners or others. Many people's relationship with themselves is downright abusive. The point of counselling is, in part, to form a relationship that is healing and nourishing. The seminal book of common factors theory, The Heart and Soul of Change (2005: 102), states that "the relationship is helpful because it provides a safe, sheltered "space" in which clients can take a deep breath, consider their problems in context, brainstorm with another person, gain perspective, examine their "bad sides," make mistakes, generate new alternatives, re-experience old wounds and problematic issues, think, analyze, recover the strength to re-confront life, and try new behaviors. In all, the relationship provides a supportive structure within which client's generative, self-healing capacities can optimally operate." The therapeutic relationship offers the ideal relationship, albeit one defined by therapeutic goals and safe and helpful boundaries. Of course every therapeutic relationship is different, for people are different. I have clients who respond best when I am challenging, others who do best with a purely supportive way of being together, others who want strong intellectual engagement, as some clients with whom I am more ironic and playful, plus some who currently need a calm authority from me for the time-being, and others who are served by pure collegiality. Part of my work is to discern what way of being and kind of relationship is most helpful for a given client. I said before that the world is a lonely place for many people, and that many have been harmed by relationships. In my essay on existential therapy and depression I discuss how our culture is somewhat toxic in this respect. I added that: "something important happened [...] in the 20th century, when Carl Rogers bravely stepped forward with a new, paradigm-breaking form of counselling. In contrast to the technical and objectifying therapies of the behaviourists and the psychoanalysts, Rogers proposed not techniques but a relationship as the core of therapy. Roger's "therapeutic relationship" is characterised by "core conditions": Empathy: The therapist must be able to understand the client's feelings and experiences from the client's point of view. The therapist should be able to see things from the client's perspective and communicate that understanding to the client. Unconditional positive regard: The therapist must accept the client without judgment, valuing them as a person, regardless of their behavior, beliefs, or attitudes. Congruence: The therapist must be authentic and genuine, openly expressing their feelings and thoughts in the therapeutic relationship. Non-directive: The therapist must allow the client to lead the therapy session, supporting the client's self-exploration and self-discovery without imposing their own agenda or advice. Active Listening: The therapist must listen to the client attentively, reflecting back what they hear, and asking open-ended questions to help the client clarify their thoughts and feelings. This philosophy of Roger's "core conditions" which he developed in the 1930s and 1940s, beautifully matches what emerged in recent decades from the common factors research. These are not scientifically-derived factors, they are not scientific ideas that we apply to people, as per the models and techniques. Look at the core conditions again and ask whether these are not simply the qualities of an ideal relationship? Do they not represent human relationships at their possible best? What would your life be like, and what would the world be like, if all our important relationships were characterised by these core conditions. People who are demanding or distrustful of themselves and others often have some objections to these core conditions, but those objections are themselves merely the expression of distrust and problems in their relationships, including with themself. Such objections reflect the experience of life in a world where human beings and human relationships are devalued. In response we can step out of that ill paradigm to the truth of our human needs, and quote the existential therapist Irvin Yalom: "it is the relationship that heals." Technique and model factors.... No one model of therapy has proven more effective than others, and yet often a model is necessary. It provides structure and focus. Hence models account for 15% of variance. There is an old Buddhist story that is relevant here, the essence of which is that if you need to get to the other bank of a river, then you need a means. It does not matter whether that means is a bridge, a boat, a raft, or a blow-up unicorn, but you need something. Models provide a shared conceptual map for the client and therapist for why the problem exists and what will be done about it. This is why people who share the medical model's view of life are generally better served by therapy in that model. They share the values and worldview of objectification, assessment and treatment, and may become frustrated at attempts by a therpist to guide them toward, say, exploration of and responsibility for their inner life. At the same time, people who are inclined toward reflection, self-awareness, personal responsibility, the inner life and a sensitivity toward meaning, are better served by a philosophical or existential model of therapy. This is how they find their way forward in the world, and more deeply it is how the world exists in their experience of it. The assumption that there is a true scientific theory of human suffering, for example psychoanalysis, for which there is one best model of treatment, is a modernist idea, a modernist myth. The idea that therapeutic models are mere structures, which appeal according to one's temperament, is perhaps a post-modern insight. Not that I am advocating for the latter, which I think is as harmful in therapy as pure modernism. The cutting edge of thought today is moving beyond modernism and post-modernism (thank goodness!) toward metamodernism. An important intellectual resource for this new paradigm is the integrational work of Ken Wilbur. Hence we can think about the place of therapeutic models in terms of Wilbur's Four Quadrant Model of knowledge, as per this video. As per my own temperament, my philosophical and existential model of therapy is most oriented to quadrant 1: the inward individual. Psychological, scientific, medicalised therapy is most oriented to quadrant 2: the objective individual. The mental health system and medical model exist at the level of quadrant 4: the objective collectivity. Jung's exploration of archetypes works at quadrant 3, the level of subjective collectivity. Of course I do think out of all four quadrants, and this is part of what Wilbur wants to suggest: not that we abandon our tempermant and mission, but that we gain a larger view and appreciation of the validity of these others categories of knowledge and experience, even as we return to our own preferred space. In the next essay I will explore how we can seperate the rest of the common factors from a models and techniques, and plug in other models, in order to explore how philosophy is a 'model' which can also be plugged in. Hope and Expectancy.... The common factors research suggests that building the client's hope is one of the essential tasks of therapy. "Clients frequently enter therapy when their efforts to improve have been unsuccessful, leaving them feeling demoralized and hopeless. In this state, there is less motivation and agency to do the work to make things better. Alleviating a client’s hopelessness and instilling renewed hope is a primary task of psychotherapy." The researchers explore this issue partly through the placebo effect. The placebo effect is very real, and I believe we need to develop a conceptualisation of it which is richer than is possible within modernism or post-modernism. Laying placeboes aside, however, from the standpoint of philosophical counselling, there is much to be fruitfully explored, and therapeutically done, in the domain of expectation and hope. A key virtue of counselling lies in cultivating hope. A key virtue of philosophical counselling lies in cultivating deep hope. Such hope includes the kind that is based on prediction of how things will turn out, but also more unconditional forms of hope that are detached from prediction, and which invite other concepts such as a love of life. I think in this connection of Albert Camus' essays collected under the title Summer in Algiers, where he evinces this love within a radically absurdist conception of life's meaning. I think also of Raimond Gaita's memoir Romulus, My Father, which happens to be set in the place where I live. In a world (including therapy) that focuses on techniques, the Holocaust survivor and existential therapist Viktor Frank said that the person who can find a Why, can find a How. For me this is the fundamental premise, promise, and impetus of philosophical counselling. A motivated human being will find a way. But it matters to us to have good motivations. Philosophy is the pursuit of both: of powerful motivations, which are worth having, which truly nourish us. A primary one among these is hope, and as I say, the love of life which is a more robust form of it. Concluding reflections.... It should be noted that the common factors literature does not propose a new therapy; it does not propose a new model and set of techniques. Rather it is research into the common factors across therapies, and its practical aim is to encourage wider and deeper integration of these factors into existing therapies. The common factors research is striking and compels one to a paradign shift. Strangely, however, while most therapists accept the soundness of this research, yet many continue to practice in the old way, focused above all on models and techniques. Hence the therapy wars continue, and counsellors move from one theoretical fashion to another. I suspect that there are various reasons for this, having above all to do with the significant emotional challenges of doing therapy. Nonetheless, the common factors should become a fundamental way for conceptualising what we do. One major limit to the research is that it focuses on therapy in the context of psychology and that discipline's medical model. I wonder what might happen if there was more inclusion of therapies focused on personal growth. Of course, there is little research done on those, and the common factors theory is based on meta-analysis of the research that is published. Nonetheless, the insights of this analysis are broadly applicable, providing a challenge to the assumptions of mainstream psychology, and validating what many of us already knew, but sharpening that knowledge for us. I return to this research throughout the years to keep me on track. What is also wonderful about it is that it provides scientific validation for any model of counselling which integrates the factors. This is what I do in my philosophical counselling: blend the common factors with transformative philosophical reflection. This enables a form of philosophical counselling which is as evidence-based as anything else. At the same time philosophical counselling goes beyond empirical evidence and psychology, into the realm of rational and creative reflection, and into meaning and value - the very things that science as a model lacks, and which as scientism it erodes. My next blog post will explore how we can blend these common factors with philosophy to create an evidence-based model of philosophical counselling. Comments are closed.
|